
Cervical Disc Herniation: Symptoms, Diagnosis, and Treatment
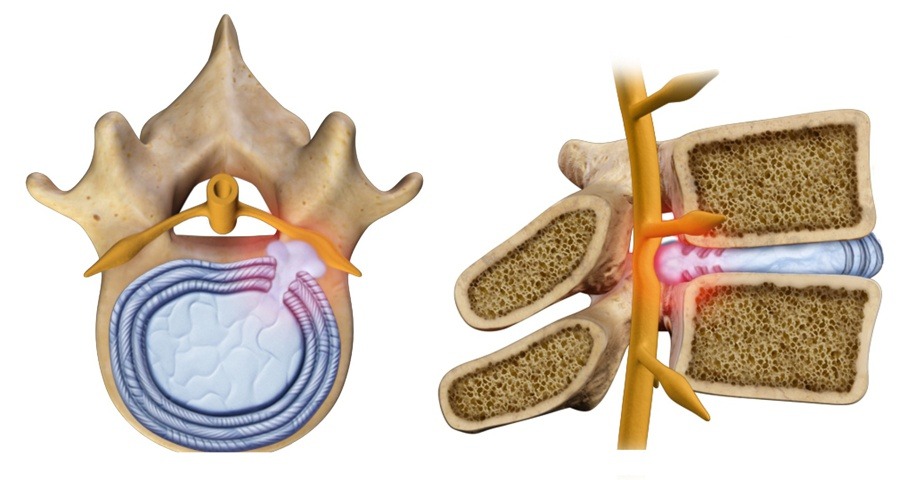
A cervical disc herniation occurs when the nucleus pulposus — the inner, gel-like portion of a cervical intervertebral disc — protrudes through a tear in the outer annulus, compressing the spinal nerves or the spinal cord.
This condition may cause neck pain, radiating arm pain (cervical radiculopathy), or, in more severe cases, cervical myelopathy, with balance difficulties, hand clumsiness, or gait disturbances.
The main causes include age-related disc degeneration, acute trauma (such as whiplash), or repetitive microtrauma.
Risk factors such as poor posture, smoking, a sedentary lifestyle, and occupations involving prolonged neck flexion (for example, office or computer work) can accelerate the degenerative process.
Diagnosis
The diagnosis is based on a in-depth clinical evaluation, and includes:
- Test dei Testing of reflexes and muscle strength
- Assessment of sensory alterations
- Evaluation of signs of spinal cord compression
MRI (Magnetic Resonance Imaging) is the gold standard examination for visualizing the herniated disc, nerve compression, and disc morphology.
In complex cases, CT myelography or electromyography (EMG) may be performed to assess nerve function.
Conservative Treatment
In 70–80% of cases, symptoms improve with non-surgical treatment within 6–12 weeks.
Treatment options include:
- Targeted physical therapy to improve posture and strengthen the cervical muscles
- Anti-inflammatory medications and muscle relaxants to reduce pain and muscle tension
- Cervical collar (temporary use) to limit painful movements (uso temporaneo) per limitare i movimenti dolorosi
- Epidural corticosteroid injections, effective in reducing radicular inflammation
During this phase, it is important to avoid sudden movements and correct posture during daily and work activities.
Surgical Treatment
La chirurgia è indicata nei casi di:
- Progressive neurological deficits (such as loss of strength or sensation)
- Cervical myelopathy
- Persistent and disabling pain that does not respond to conservative treatments
The most common procedure is anterior cervical discectomy and fusion (ACDF), which allows surgeons to remove the herniated disc, relieve nerve compression, and stabilize the spine, with a success rate exceeding 85%.
A modern alternative is cervical disc replacement (CDR), which preserves segmental mobility and reduces the risk of adjacent level degeneration.
Minimally invasive posterior techniques, such as endoscopic foraminotomy, enable targeted decompression through smaller incisions and faster recovery.
In complex cases involving multiple levels, hybrid surgery may be recommended, combining fusion and disc prosthesis to optimize both stability and motion.
Recovery and Rehabilitation
The post-operative rehabilitation pathway is essential for optimal recovery.
It includes:
- Progressive physical therapy to restore mobility and strength
- Ergonomic education, with attention to workstation setup and computer use
- Attività a basso impatto (camminate, esercizi di stretching, nuoto)
- Weight control and smoking cessation
Post-operative complications, such as dysphagia or transient hoarseness, occur in 5–30% of cases but tend to resolve spontaneously within a few weeks or months.
Conclusions
Cervical disc herniation is a common condition but can be effectively managed with personalized treatments.
An early evaluation by a spine specialist helps identify the most appropriate strategy — conservative or surgical — based on the severity of symptoms, the degree of nerve compression, and the patient’s goals.
The ultimate goal is to preserve cervical function, relieve pain, and ensure a healthy spine in the long term.