
Lumbar Spinal Stenosis: Symptoms, Diagnosis, and Treatment
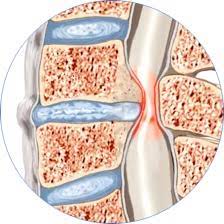
The lumbar spinal stenosis (LSS) è una condizione caratterizzata dal narrowing of the spinal canal or neural foramina in the lower back. This narrowing, often due to processi degenerativi legati all’età (come ispessimento dei legamenti, formazione di osteofiti o protrusioni discali), può comprimere i nervi spinali o la cauda equina, causing a series of typical symptoms.
Il disturbo più comune è la claudicatio neurogena, a pain or tingling in the legs that worsens when walking or standing and improves by sitting or leaning forward. Other symptoms may include dolore lombare, ridotta mobilità e, nei casi più gravi, changes in bowel or bladder function. Risk factors include l’invecchiamento, il sovrappeso, la predisposizione genetica and all attività lavorative che comportano sforzi ripetuti sulla colonna vertebrale.
Diagnosis
The diagnosis is based on a in-depth clinical evaluation, comprendente l’anamnesi dettagliata, l’esame obiettivo con osservazione del passo e test dei riflessi. L’Magnetic resonance imaging (MRI) rappresenta l’esame di riferimento per valutare la larghezza del canale spinale e l’eventuale compressione nervosa. In casi specifici, si possono utilizzare CT myelography or dynamic radiographs per analizzare la stabilità vertebrale. Inoltre, il Swiss Spinal Stenosis Questionnaire (SSSQ) aiuta a quantificare la gravità dei sintomi e le limitazioni funzionali.
Treatment
Il primo approccio è conservative, and includes:
- Physiotherapy to improve posture and strengthen the core muscles
- Anti-inflammatory drugs to reduce pain and inflammation
- Modifiche delle attività quotidiane per ridurre lo stress sulla colonna
- Epidural corticosteroid injections to relieve symptoms in resistant cases
When non-surgical therapies do not provide benefit, surgical decompression may be considered to relieve the compressed nerve structures. The most commonly used techniques include traditional laminectomy or minimally invasive laminotomy, which reduce pain and improve quality of life. In selected cases, interspinous distraction devices (such as X-Stop) may be used to prevent vertebral instability.
Spinal fusion, on the other hand, is reserved for patients with associated spinal instability or degenerative spondylolisthesis.
Prognosis and Rehabilitation
After surgery, 70–80% of patients report a significant improvement in pain and quality of life, although full recovery may take several months. Post-operative rehabilitation, together with an active lifestyle, weight management, and low-impact physical activity, is essential to maintain long-term results.
An early evaluation by a spine specialist allows for the development of a personalized treatment plan, balancing symptom severity, anatomical factors, and the patient’s goals, with the aim of preserving long-term spinal health.